Clinician teaching
MASLD: Pathophysiology to FibroScan
A primary-care teaching deck on why steatosis identifies metabolic exposure while fibrosis changes risk and management.
Learning objectives
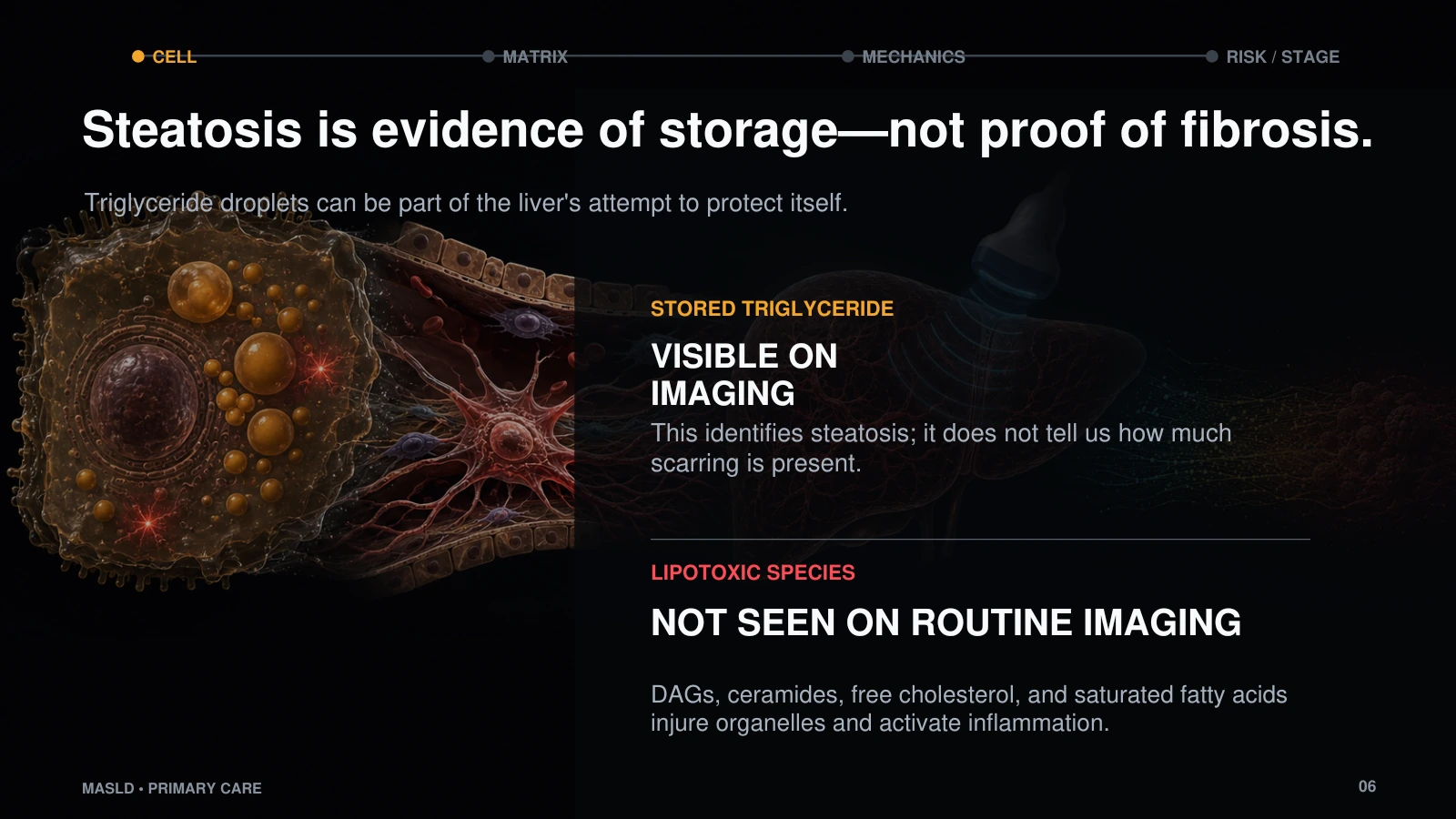
- Separate steatosis as metabolic exposure from fibrosis as the finding that changes prognosis and management.
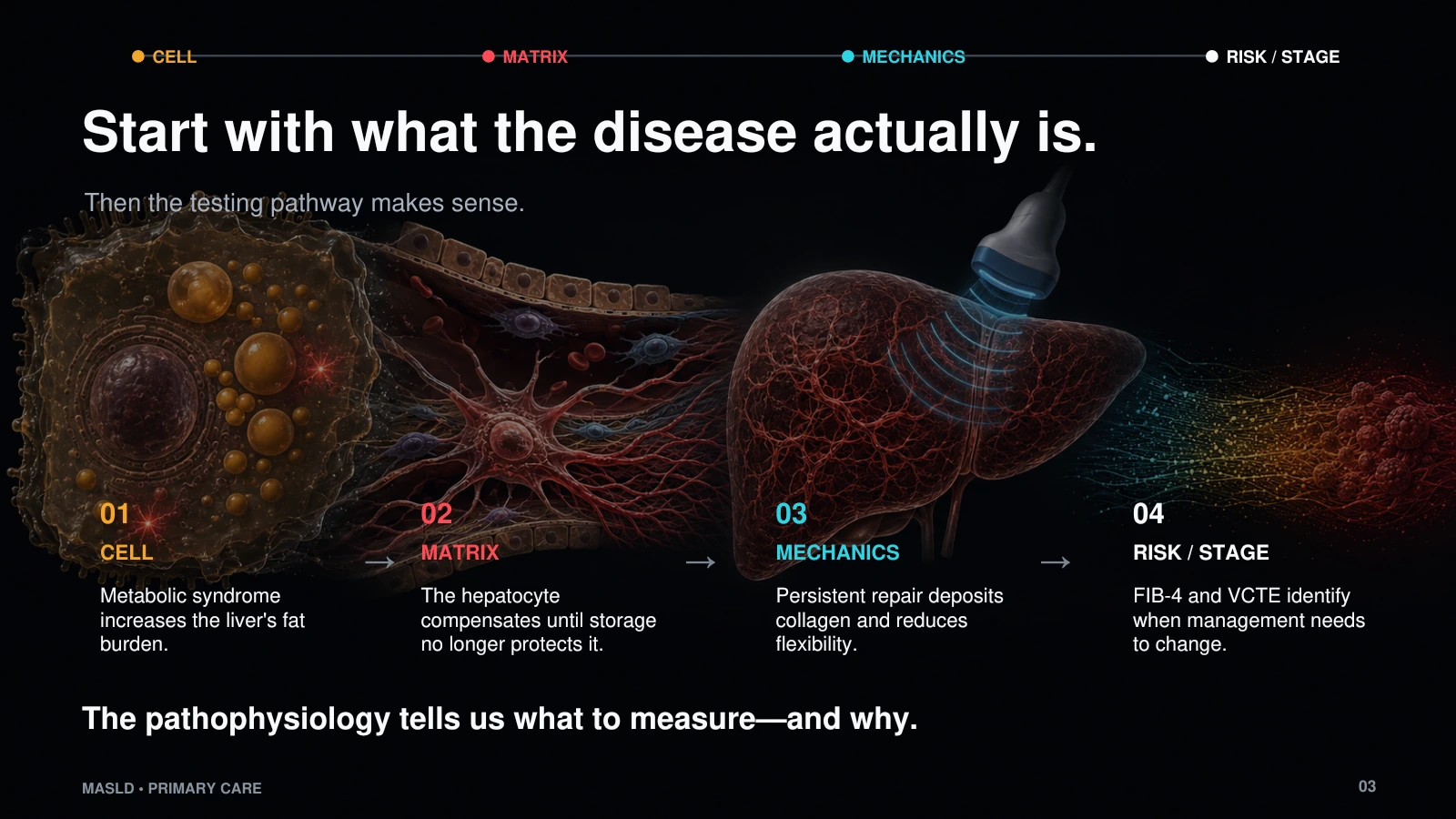
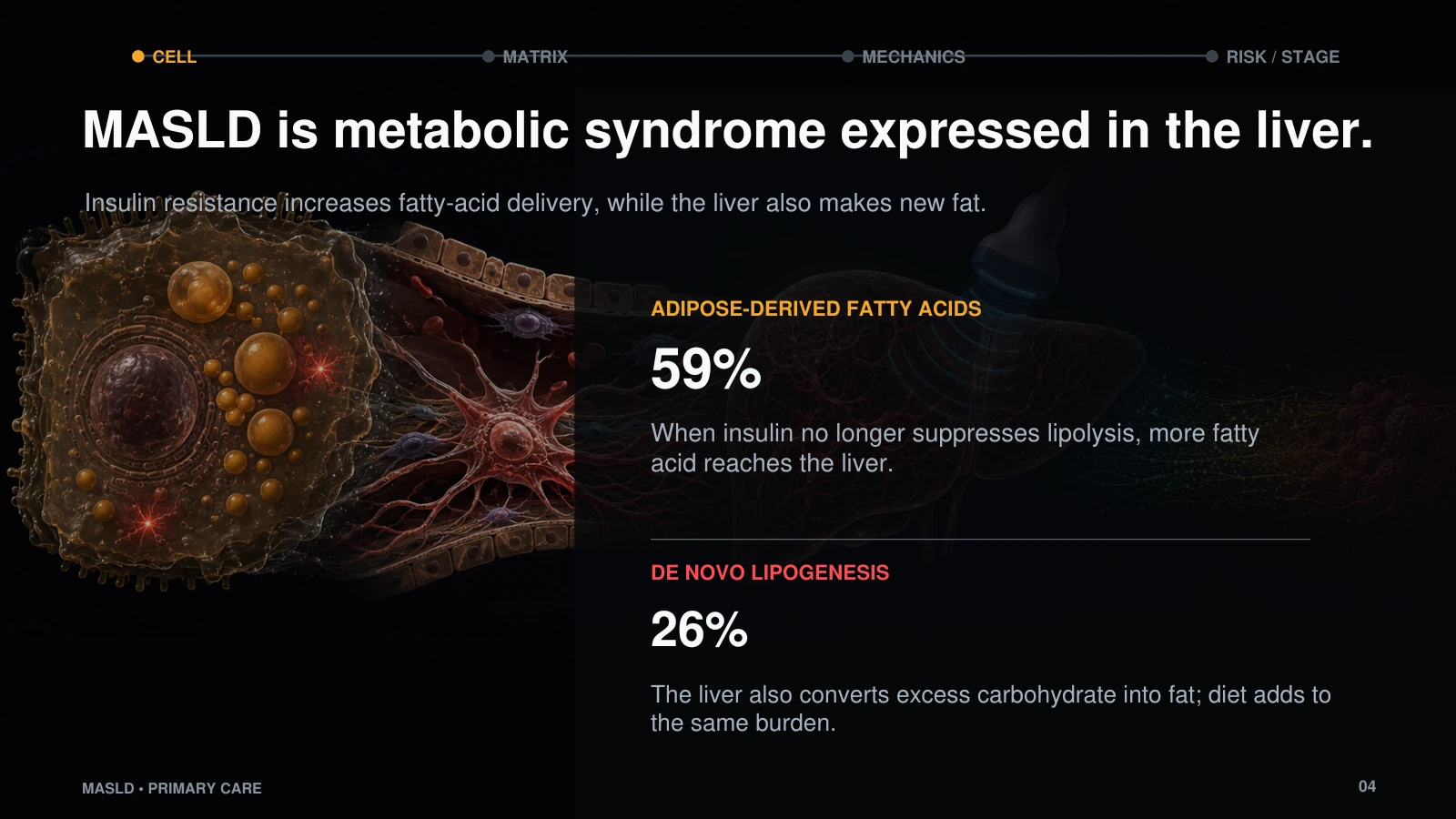
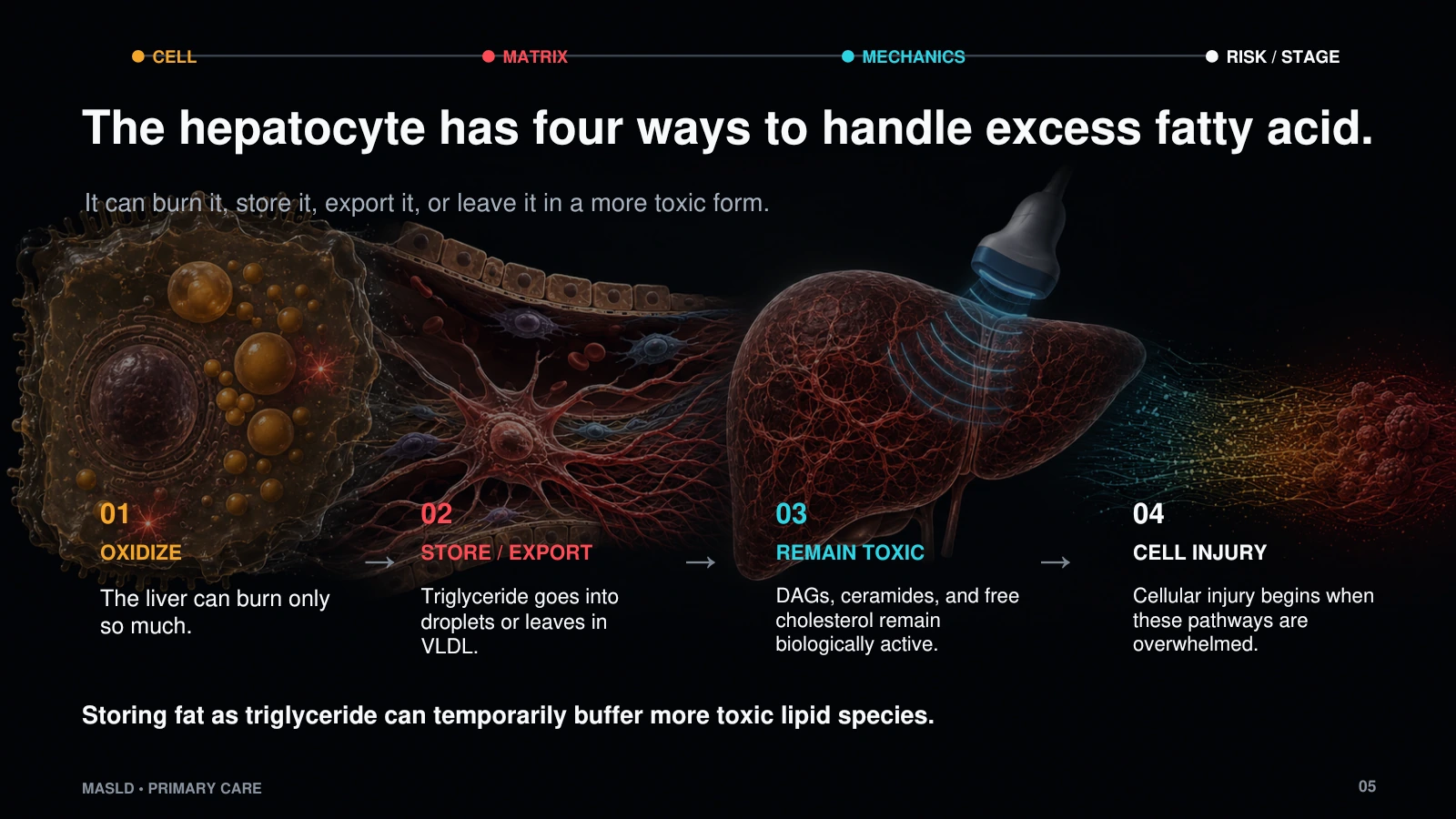
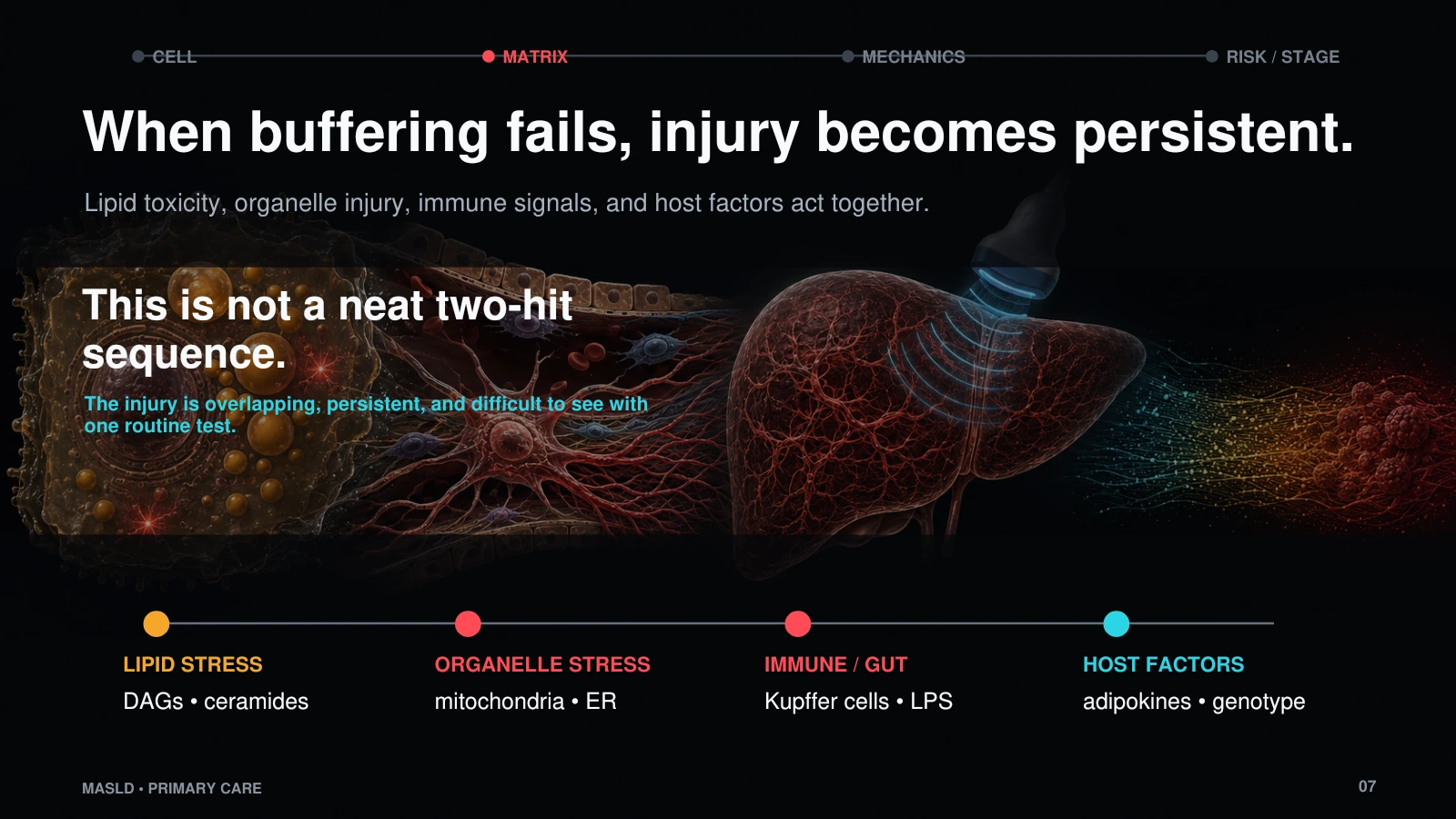
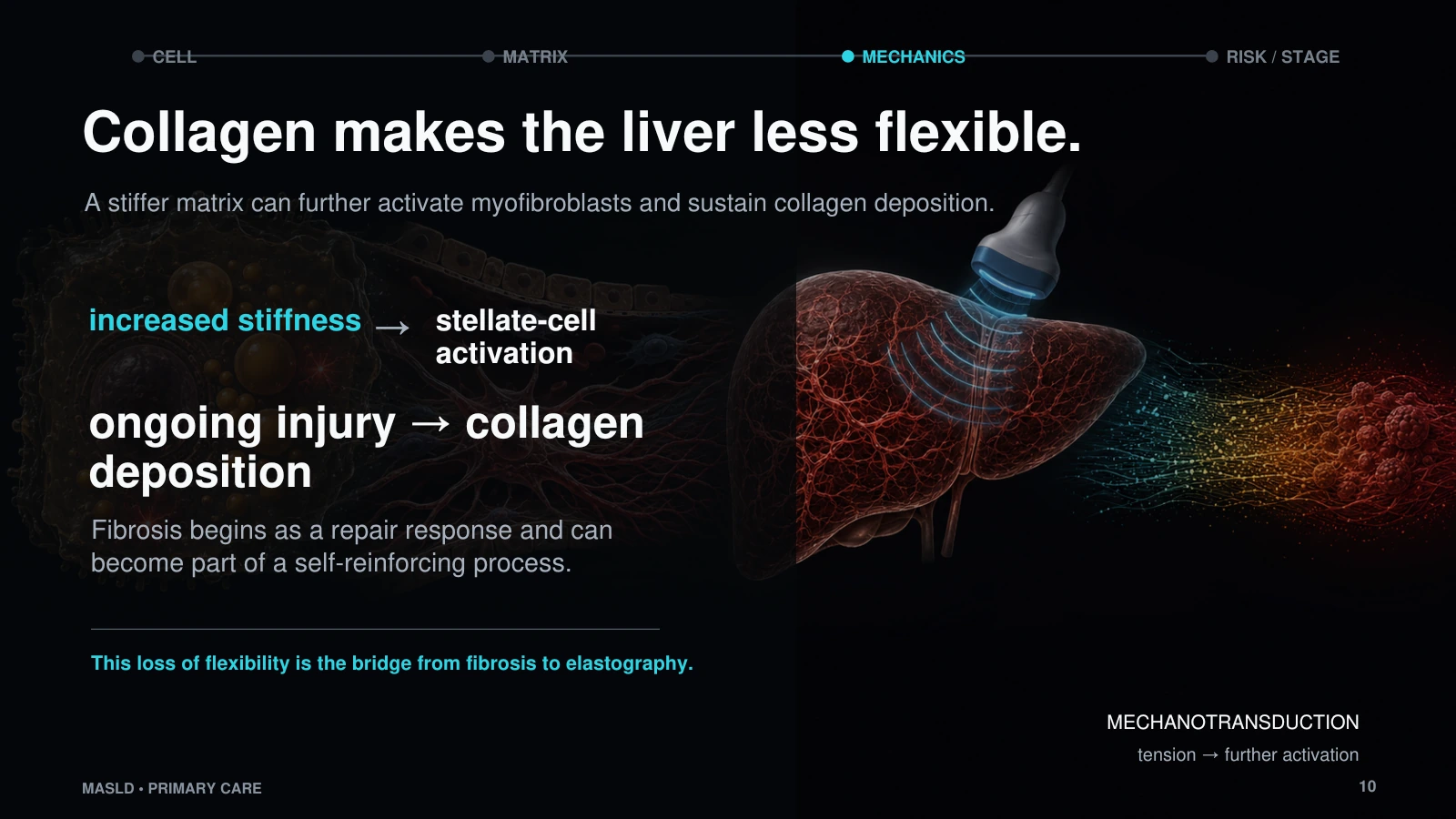
- Explain how metabolic overload overwhelms hepatocyte resilience and turns repair into collagen deposition.
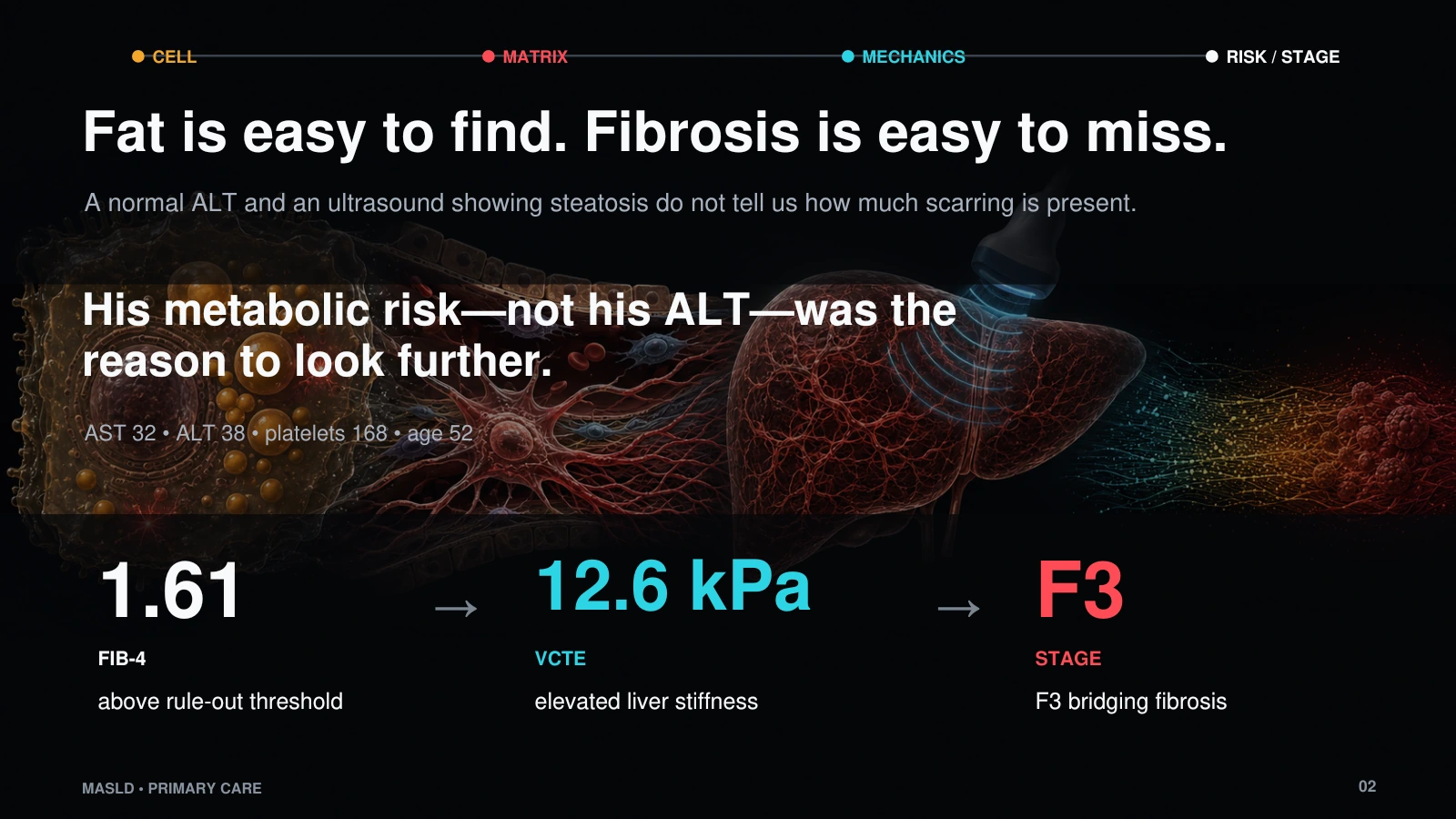
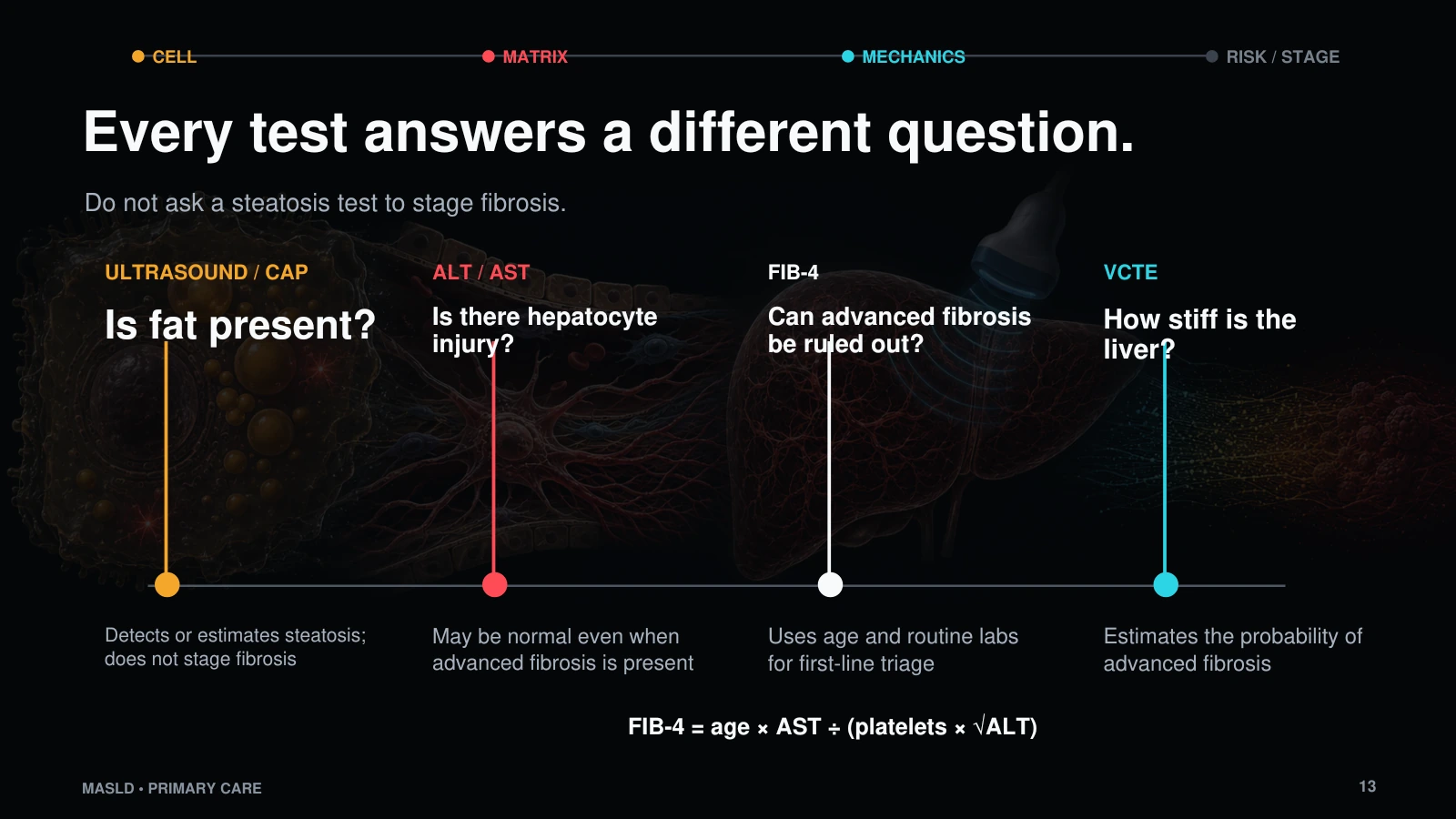
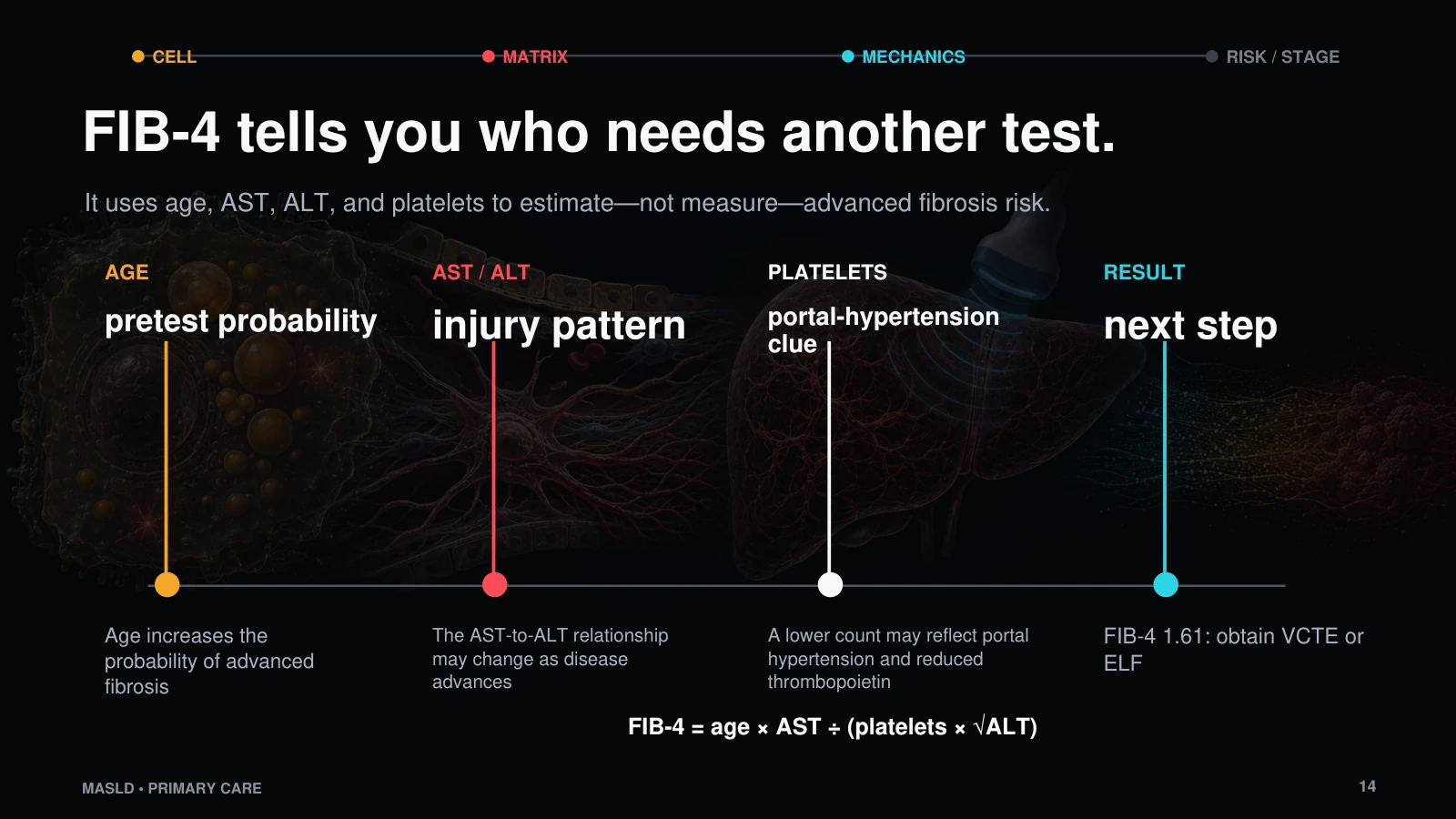
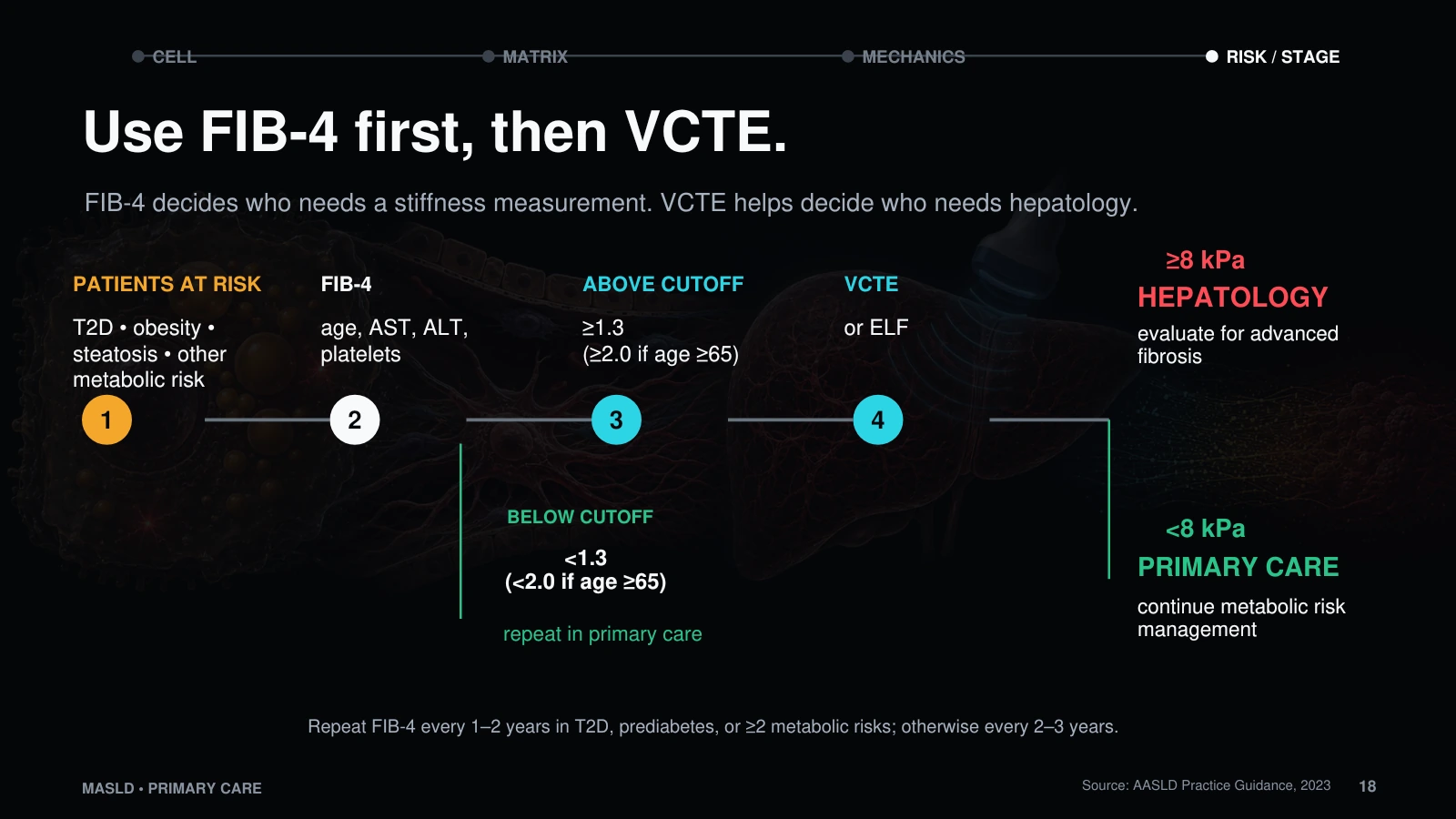
- Use FIB-4 as a first-pass triage tool and elastography as the next fibrosis-risk assessment.
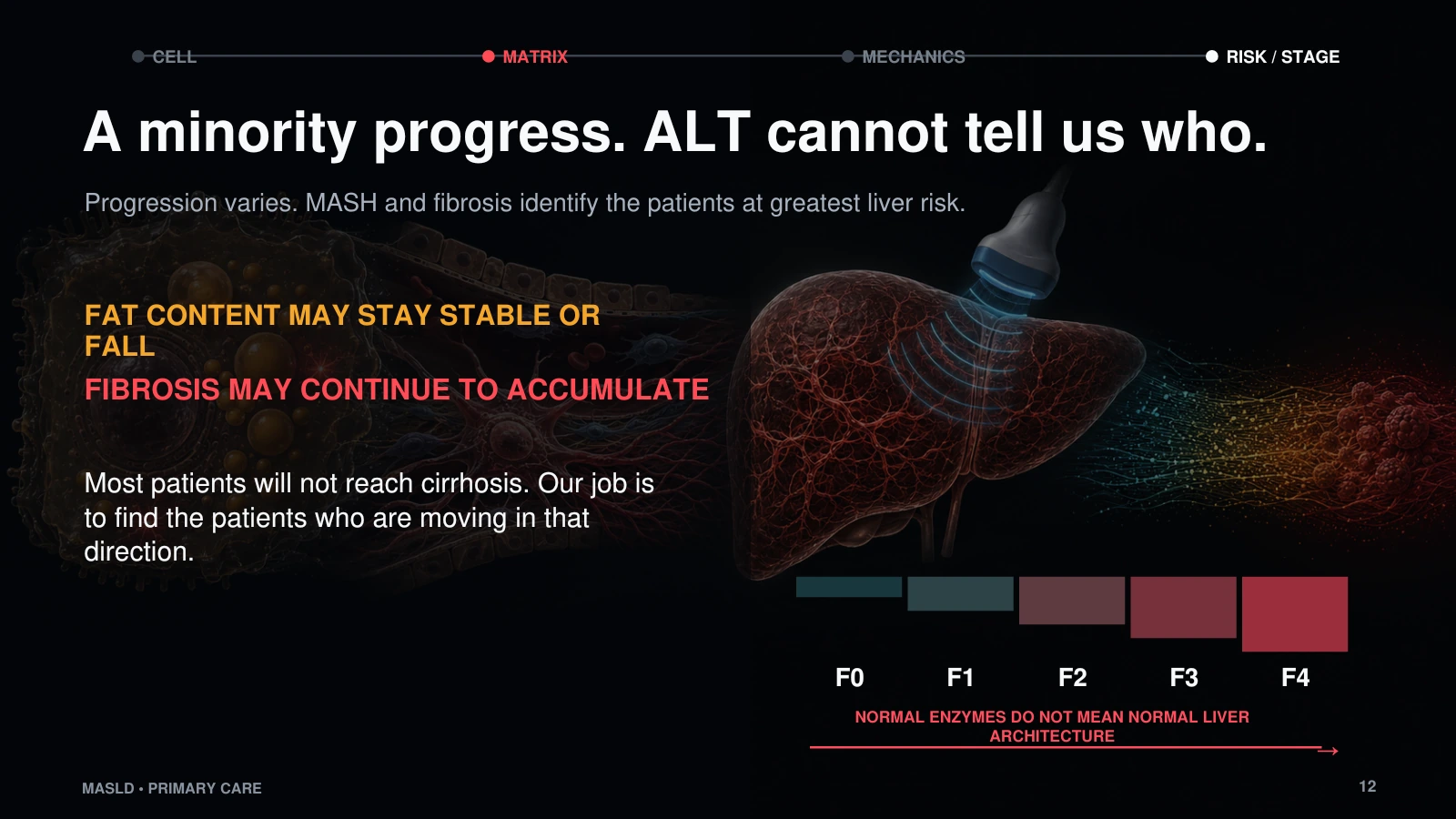
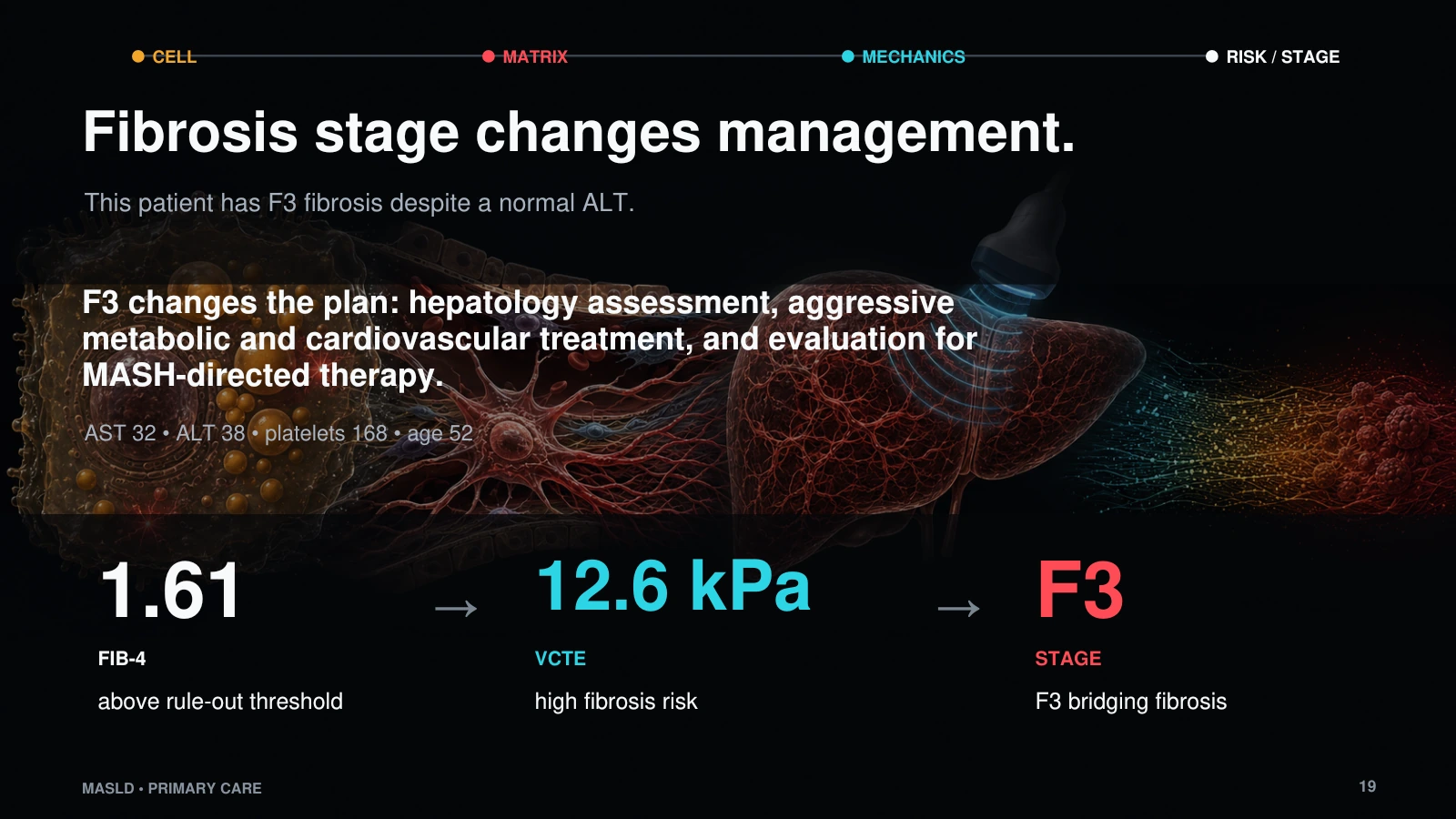
- Recognize when fibrosis stage, not ALT alone, should change the clinical plan.
Major teaching sequence
- Start with the clinical miss: ultrasound finds fat, but the patient who matters is the one whose fibrosis is already advancing.
- Return to normal hepatic resilience: the liver can oxidize, export, and store fat before injury becomes persistent.
- Follow overload into hepatocyte stress, inflammatory signaling, stellate-cell activation, and collagen deposition in the space of Disse.
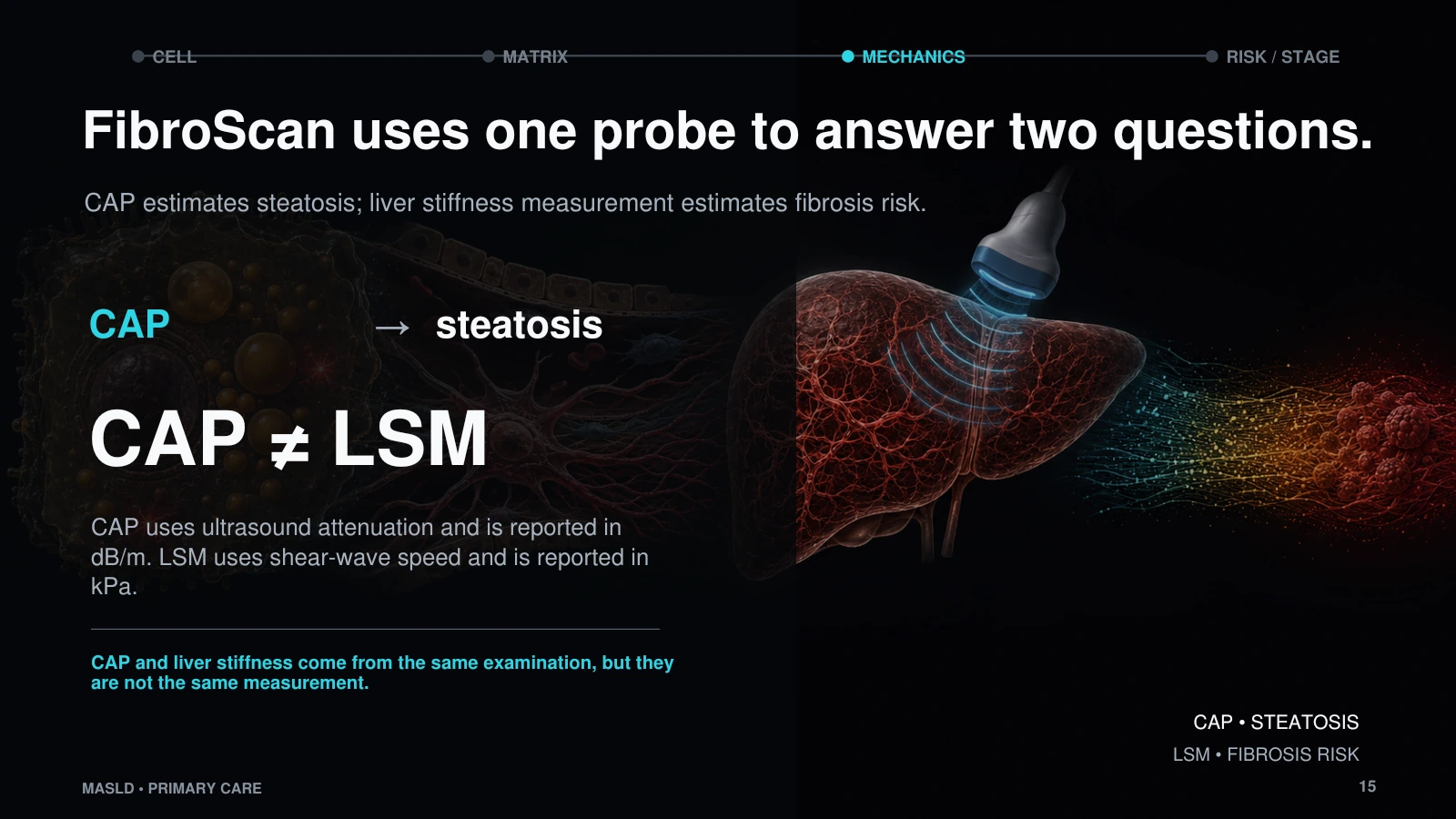
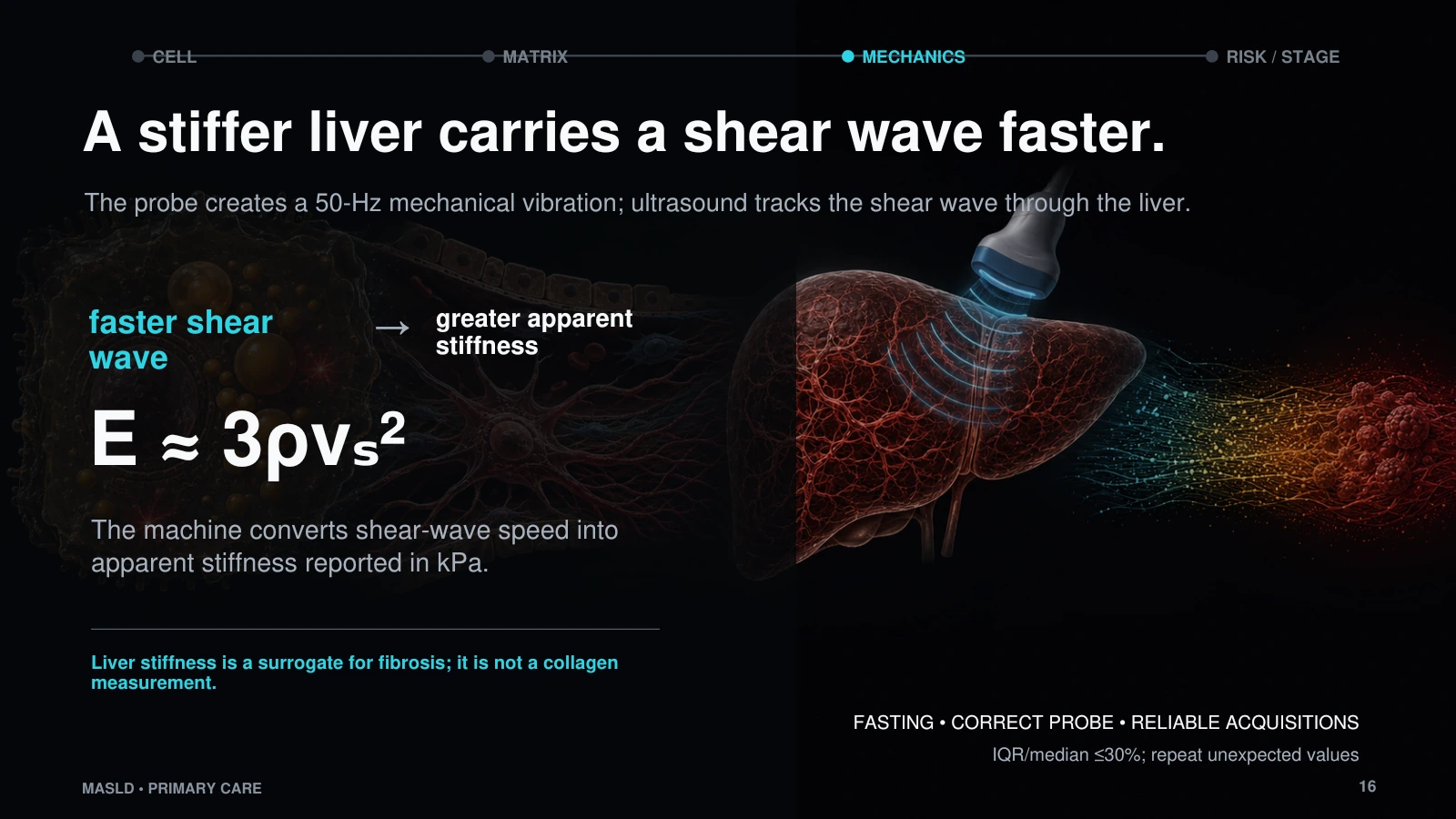
- Make the invisible measurable: FIB-4 estimates who needs another test; VCTE estimates liver stiffness and fibrosis probability.
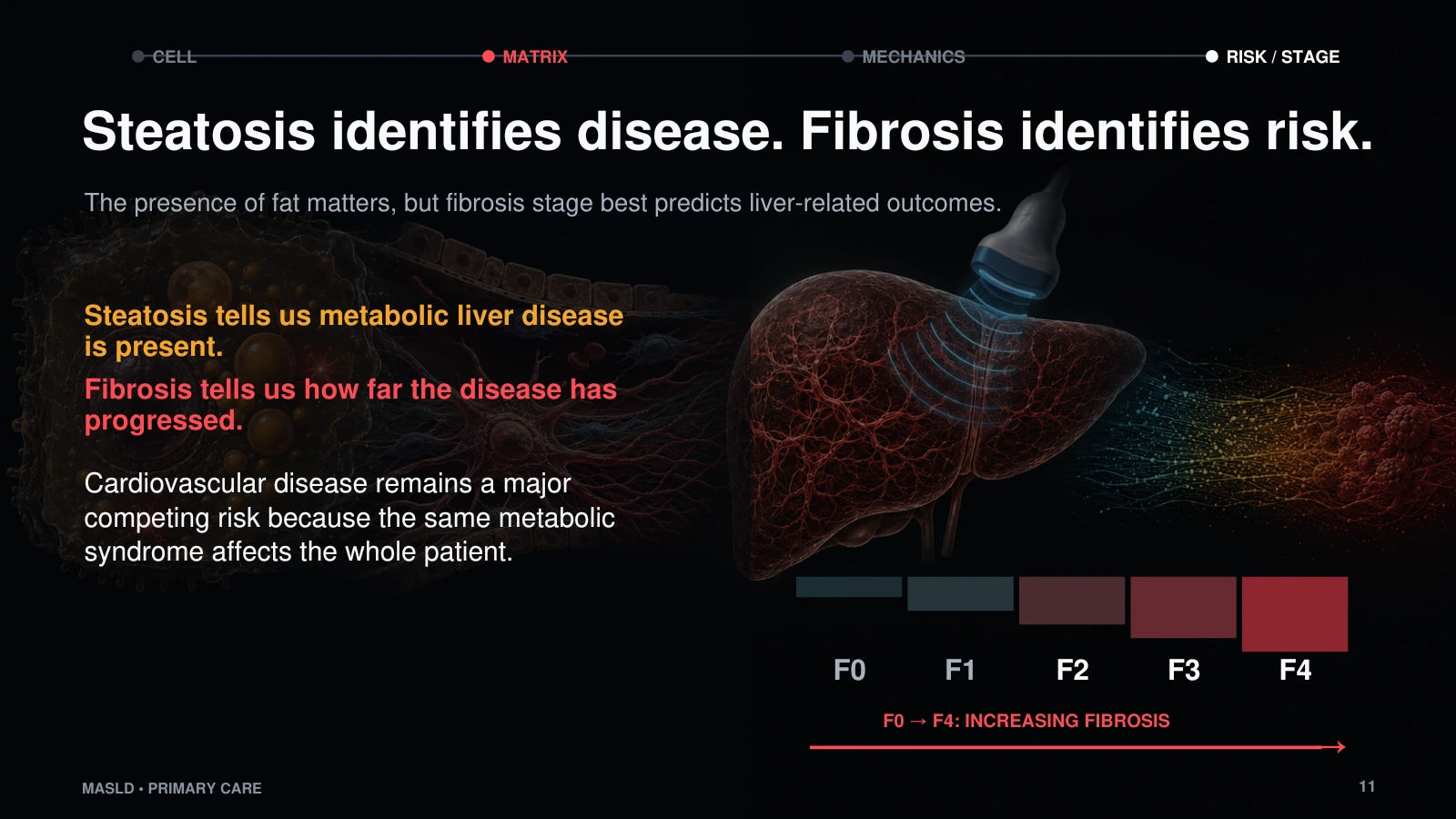
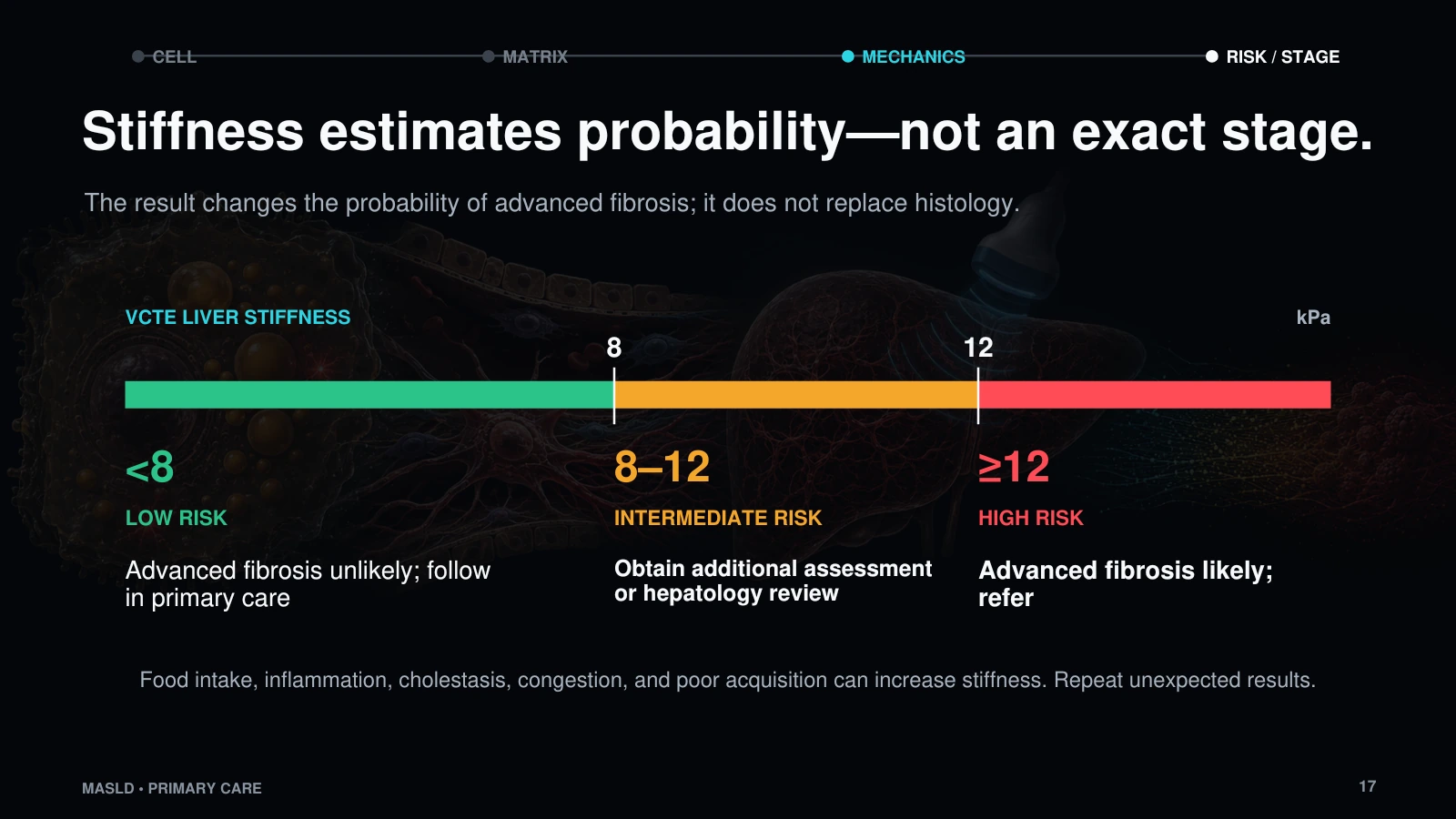
- Close with risk stratification: steatosis identifies the disease process, while fibrosis identifies the management-changing risk.
Slide viewer


References
- AASLD Practice Guidance on clinical assessment and management of NAFLD/MASLD, including 2024 and 2025 MASLD therapy updates.
- AASLD noninvasive liver disease assessment guidance for blood-based and imaging-based fibrosis assessment.
- FDA approval materials for resmetirom in adults with noncirrhotic NASH/MASH with moderate to advanced fibrosis.
- FDA approval materials for semaglutide in adults with MASH and moderate-to-advanced fibrosis.
- AASLD practice guidance on portal hypertension and varices in cirrhosis.